
Scoliosis and Back Pain
What is Scoliosis?
 You have probably heard of, or at least known someone diagnosed with, scoliosis, but what exactly is this condition? Scoliosis is a spinal deformity that involves sideways curvature of the vertebrae.1 While this condition can affect anyone from infants to adolescents, it is overwhelmingly most prevalent in those older than 10 years of age.1 Within this adolescent age group, approximately 1-3% will be diagnosed with scoliosis, usually of unknown origin (idiopathic).2 Females are more commonly diagnosed and, interestingly, there is also a preference for right-sided curvature.2
You have probably heard of, or at least known someone diagnosed with, scoliosis, but what exactly is this condition? Scoliosis is a spinal deformity that involves sideways curvature of the vertebrae.1 While this condition can affect anyone from infants to adolescents, it is overwhelmingly most prevalent in those older than 10 years of age.1 Within this adolescent age group, approximately 1-3% will be diagnosed with scoliosis, usually of unknown origin (idiopathic).2 Females are more commonly diagnosed and, interestingly, there is also a preference for right-sided curvature.2
Types/Causes of Scoliosis
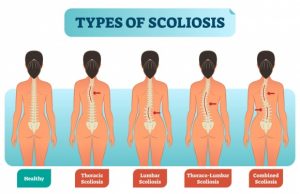
There are several broad categories of scoliosis, which include congenital, neuromuscular, and idiopathic.
Congenital Scoliosis
This type consists of skeletal abnormalities that are present at birth, largely due to malfunctions during the development of the vertebrae.1 Because other organ systems are also developing in utero at this same time, patients with this type of scoliosis may also have other neurological, cardiovascular, or genitourinary abnormalities.1 This condition is usually identified on fetal ultrasound, and in most mild cases will resolve spontaneously.3
Syndrome-Related Scoliosis
This type of scoliosis is associated with pre-existing neuromuscular conditions or other syndromes. In these cases, the accompanying condition will have its own symptoms in addition to the characteristic scoliosis structure.1 Several of these syndromes include cerebral palsy, Duchenne muscular dystrophy, and Marfan syndrome.1
Idiopathic Scoliosis
Idiopathic scoliosis makes up the majority of scoliosis cases that a physician encounters.1 Unfortunately, this type is mostly a diagnosis of exclusion, meaning that it simply does not fit into any other category. Although the inheritance pattern is obscure, there may be a genetic component to this condition, since nearly 25% of patients also have a relative with scoliosis.3 Patients with idiopathic scoliosis are further classified depending on their age at presentation, with the majority of cases (89%) being adolescents (AIS).4 This age corresponds with rapid adolescent growth and, if the condition presents before this growth spurt, has the potential to cause severe trunk deformities.1
Diagnosis and Treatment of Scoliosis
Diagnosis begins by thoroughly investigating primary causes for the deformity and/or ruling out other diagnoses. Most patients with idiopathic scoliosis are recognized by friends or family due to a deformity, which could include asymmetry of the shoulders, waist, or rib cage.3 This condition was traditionally thought to be non-painful, but research has shown that associated back pain is not unusual.5
Treatment
Treatments for scoliosis are specified based on the scoliosis sub-type, the magnitude of spinal curvature, and how many years of growth the patient has remained, among other factors.1 For example, if you have a curve magnitude of less than 10°, you are likely a low risk for progression and are considered a normal variant.6 Those with a curve greater than 50° at presentation are high risk for further progression.6 Even higher risk are adolescents with years of growth left, since this leaves room for the spinal curve to grow and worsen.6
Treatment Options for Scoliosis
 Treatment options include observation, physiotherapy, and bracing, with the general goal to keep curves under 50° by the time of maturity.1 If this is not possible, surgery may be implicated. Physiotherapy is thought to be a crucial element of conservative scoliosis treatment for mild deformities; although the evidence is limited, some studies have shown moderate efficacy with this intervention when added to existing rehabilitation.7,8 The goal of physiotherapy is to stabilize the spine and trunk and prevent further functional disabilities.9 For skeletally immature patients, those with a mild curve are usually recommended observation, while those with more moderate curves (25° to 50°) are often prescribed a brace.1,10 It should be noted, however, that bracing does not improve or correct the curve, but rather attempts to prevent worsening.10 If the curve continues to progress at this point, surgical correction may be considered to avoid lung/heart problems. Surgery is normally performed during adolescence, but new techniques have allowed for correction during early adulthood as well.1
Treatment options include observation, physiotherapy, and bracing, with the general goal to keep curves under 50° by the time of maturity.1 If this is not possible, surgery may be implicated. Physiotherapy is thought to be a crucial element of conservative scoliosis treatment for mild deformities; although the evidence is limited, some studies have shown moderate efficacy with this intervention when added to existing rehabilitation.7,8 The goal of physiotherapy is to stabilize the spine and trunk and prevent further functional disabilities.9 For skeletally immature patients, those with a mild curve are usually recommended observation, while those with more moderate curves (25° to 50°) are often prescribed a brace.1,10 It should be noted, however, that bracing does not improve or correct the curve, but rather attempts to prevent worsening.10 If the curve continues to progress at this point, surgical correction may be considered to avoid lung/heart problems. Surgery is normally performed during adolescence, but new techniques have allowed for correction during early adulthood as well.1
Recommendations for Managing Scoliosis
Start Intervention Early
As mentioned earlier, patients with a greater curve magnitude at presentation are more at risk for worsening of the condition.6 Thus, early intervention is critical to try to minimize progression so patients can maintain quality of life.
Stay active with sports and activity
A reduction in physical activity can be detrimental to the overall physical and mental well being of any patient, but especially adolescent scoliosis patients.11 Many experts recommend that activity for those with scoliosis should be similar to those without scoliosis (i.e. 60 minutes of activity daily) given physician approval.12 However, you should take caution when engaging in contact sports, especially after surgery, and should also follow the recommendations of your personal physician.
Maintain a positive outlook
Scoliosis can be both a physically and emotionally uncomfortable condition by altering one’s appearance and self-image. Because of this, it can be disheartening to hear that your best treatment option is simply an observation. However, we hope you will not become discouraged – maintaining a positive outlook is critical to prevent the psychological and emotional distress that many patients report.13 Surrounding yourself with friends, family, and loved ones who can support you through the process can ease the burden you might be experiencing.
Stretch and maintain good core strength
For some athletes, training for balance and posture control, core strengthening, and increasing flexibility have been proven useful in preparing them to return back to their sport after spinal surgery.14 If you are neither an athlete nor recovering from surgery, stretching, and practicing core strengthening exercises is still critical for optimizing your functional abilities. Lucky for you, it just so happens that we have rounded up some of our favorite exercises below that might help you manage your scoliosis.
The Best Exercises to Manage Scoliosis and to Prevent it from Progressing
Childs pose with a Lat Stretch
Goal: Lengthen and stretch the latissimus dorsi (side muscles) and spinal erector muscles to better neutralize your spine
Instructions:
- Begin with all fours on the ground
- Keeping your shoulders out in front of you, slowly move your butt backward towards your heels
- The further back you can stretch, the more you will target your spinal erector muscles
- While maintaining the stretch, slowly walk your hands to the left/right to isolate one side
Thoracic Stretch for Scoliosis
Goal: Thoracic scoliosis can directly affect the latissimus dorsi, so strengthening these muscles can help combat the condition
Instructions:
- Stand in neutral position with knees slightly bent
- Using a step stool or stair-step to the left of you, place your left foot on the step
- The step should be just a few inches off the ground so that the toes of the right foot can just barely touch the ground
- Extend your right arm over your head and slowly bend to the left
- You should feel the stretch in your right torso
- Repeat on the other side


Side Planks with Hip Lifts
Goal: To strengthen the muscles on the side of the spine
Instructions:
-
-
- Begin sitting on the ground, then turn so you are laying on one side
- Legs should be stacked and extended. The elbow on the ground should remain underneath your shoulder
- With your opposite arm raised towards the ceiling, lift your torso off the ground into a side plank position
- For a modification, you may keep your knees bent and on the ground
- Slowly pulse, lifting your hips towards the ceiling
- Imagine a string attached to your hips that was pulling them upwards
-
Bridges with a Pelvic Tilt
Goal: Strengthen the intra-abdominal muscles to help stabilize the spine
Instructions:
-
-
- Start by laying on the ground with your back on the floor
- Both feet on the ground and knees bent
- Assume a posterior pelvic tilt
- Imagine a string pulling your belly button and lower abdomen into the ground
- While maintaining the posterior pelvic tilt, press your hips upwards and off the ground so that your butt, hips, and lower torso are elevated off the ground
- Try to maintain a straight line from your torso to your knees
- Squeeze the abdominals and glutes
- Hold this position for several seconds, then release back down
- Repeat several repetitions
- Start by laying on the ground with your back on the floor
-
Bird Dogs on a Swiss Ball
Goal: To strengthen the muscles of the spine and improve the stability of the core
Instructions:
-
-
Position yourself stomach-down on an exercise ball, with the ball underneath your hips
- Place your hands out in front of the ball, shoulder-width apart, and toes touching the ground behind you
- Raise one arm straight in front of you and simultaneously lift the opposite leg behind you
- Focus on using your lower back muscles to lift the arm and leg
- Return both arm and foot to starting position
- Raise the other arm and the other leg
- Make sure to maintain a tight core during the exercise
-

Conclusion
Because the causes of scoliosis are largely unknown and treatment options are limited, it can be frustrating to deal with this debilitating condition. However difficult it may seem, continuing to remain active and taking care of your body, physical, emotionally, and mentally, are the most important aspects of managing your scoliosis.
Works Referenced
- Janicki, J.A., and Alman, B. (2007). Scoliosis: Review of diagnosis and treatment. Paediatrics & Child Health 12, 771.
- Menger, R.P., and Sin, A.H. (2018). Adolescent and Idiopathic Scoliosis (StatPearls Publishing).
- Choudhry, M.N., Ahmad, Z., and Verma, R. (2016). Adolescent Idiopathic Scoliosis. The Open Orthopaedics Journal 10, 143–154.
- Riseborough, E.J., and Wynne Davies, R. (1973). A genetic survey of idiopathic scoliosis in Boston, Massachusetts. Journal of Bone and Joint Surgery – Series A 55, 974–982.
- Ramirez, N., Johnston, C.E., and Browne, R.H. (1997). The prevalence of back pain in children who have idiopathic scoliosis. Journal of Bone and Joint Surgery – Series A 79, 364–368.
- Wong, H.K., and Tan, K.J. (2010). The natural history of adolescent idiopathic scoliosis. Indian Journal of Orthopaedics 44, 9–13.
- Weiss, H.R., and Klein, R. (2006). Improving excellence in scoliosis rehabilitation: A controlled study of matched pairs. Pediatric Rehabilitation 9, 190–200.
- Schreiber, S., Parent, E.C., Moez, E.K., Hedden, D.M., Hill, D., Moreau, M.J., Lou, E., Watkins, E.M., and Southon, S.C. (2015). The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner.” Scoliosis 10.
- Ridderbusch, K., Spiro, A.S., Kunkel, P., Grolle, B., Stücker, R., and Rupprecht, M. (2018). Strategies for Treating Scoliosis in Early Childhood. Deutsches Arzteblatt International 115, 371–376.
- Nachemson, A.L., Peterson, L.E., Bradford, D.S., Burwell, R.G., Duhaime, M., Edgar, M.A., Eppig, M.M., Gardner, A.D.H., Kehl, D.K., Lidstrom, J., et al. (1995). Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. Journal of Bone and Joint Surgery – Series A 77, 815–822.
- Kakar, R.S., Simpson, K.J., DAS, B.M., and Brown, C.N. (2017). Review of Physical Activity Benefits and Potential Considerations for Individuals with Surgical Fusion of Spine for Scoliosis. International Journal of Exercise Science 10, 166–177.
- Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report, 2008. Washington, DC: US Department of Health and Human Services; 2008. pp. A1–H14.
- Sanders, A.E., Andras, L.M., Iantorno, S.E., Hamilton, A., Choi, P.D., and Skaggs, D.L. (2018). Clinically Significant Psychological and Emotional Distress in 32% of Adolescent Idiopathic Scoliosis Patients. Spine Deformity 6, 435–440.
- Cox SM, Dingle CR. Adolescent Idiopathic Scoliosis in a College Golfer. Int J Athl Ther Train. 2011;16(2):8–11.
Disclaimer: The information provided in this post is for educational purposes only. This is not a substitute for a medical appointment. Please refer to your physician before starting any exercise program.